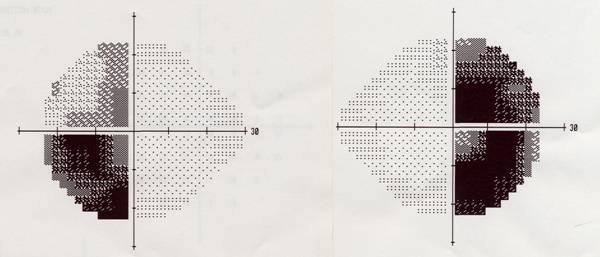
From Lewis Blevins, MD – These images show the serial visual fields in a patient with a pituitary tumor. The blackened parts illustrate what the patient CANNOT see as if they were our very own eyes.
 Light is brought in by the eyes and hits the retina. The retina is basically a very specialized layer of nervous tissue in the back of the eye that sends projections through the optic nerves which meet up at the optic chiasm and then separate forming the optic tracts. The optic chiasm is located just above the pituitary fossa. Within the optic chiasm the fibers on the inner part of the retina cross to the other side. The fibers on the outer part stay on the same side. The inner parts of the retina “see” the outer or peripheral vision. The outer parts of the retina see the vision in the central or “out front” visual fields.
Light is brought in by the eyes and hits the retina. The retina is basically a very specialized layer of nervous tissue in the back of the eye that sends projections through the optic nerves which meet up at the optic chiasm and then separate forming the optic tracts. The optic chiasm is located just above the pituitary fossa. Within the optic chiasm the fibers on the inner part of the retina cross to the other side. The fibers on the outer part stay on the same side. The inner parts of the retina “see” the outer or peripheral vision. The outer parts of the retina see the vision in the central or “out front” visual fields.
In the first panel, there is blindness in the outside parts, or classic bitemporal hemianopsia. This happens because a pituitary tumor pressing on the under surface of the optic chiasm affects the crossing fibers from the inner parts of the retina which see light in the periphery. Depending on the site of the tumor, and where the visual pathways cross in relation to the sella turcica, patients may have the classic loss of peripheral vision, or may lose vision in one eye, or on the same side in both eyes. There may also be a loss of the upper lateral or outside vision in patient’s diagnosed at an early stage. Many patients go on to have profound visual abnormalities before they are diagnosed. Some of the early signs are that people will bump into doorways or cabinets, or even other people in the hallway, hit curbs or mail boxes with their cars, and even sideswipe other vehicle’s while driving. Also, affected patients often have trouble driving at night because they did not see red (tail lights) as well when they have visual abnormalities due to pituitary disease.
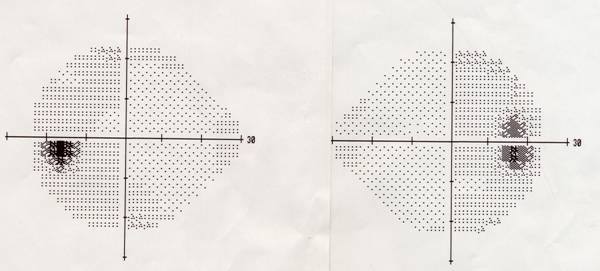
The middle images show the visual fields having improved after about one week of treatment with cabergoline to regress what proved to be a large prolactinoma.
The third panel shows complete normalization of the fields of vision after about 3 months of treatment.
Although this patient’s prolactin level fell from about 2000 to 200 after 6 months of treatment with maximum dose cabergoline, and even though his tumor regressed only a slight amount but enough to result resolution of his visual deficits, it was still rather large causing headaches and hypopituitarism. Thus, he ultimately underwent transsphenoidal surgery which restored his pituitary function to normal, lowered his prolactin to 150, and subsequent treatment with cabergoline normalized his prolactin.
© 2014 – 2016, Pituitary World News. All rights reserved.